
For nearly 30 years, Javier Aceves worked as a pediatrician in Albuquerque, New Mexico, focusing primarily on disadvantaged families. His approach was holistic: along with treating children, he did outreach with teens, and helped children’s parents with everything from addiction to learning how to be a supportive caregiver. For all the programs he helped develop, the patterns he kept seeing haunted him. He could treat young kids’ medical problems, but as they grew up, “we’d lose them to violence,” he says. Kids died all the time, by homicide or suicide.
One child he treated, Juan*, was born to a single mom who was addicted to alcohol. Juan was a smart kid who’d had a tough time: He and his siblings were periodically removed from their mother and shuttled to different relatives, and they lived in near-constant uncertainty and poverty. When Juan’s mother was in charge of her kids, she would sometimes come to Aceves, angrily asking for medication to deal with Juan’s behavior.
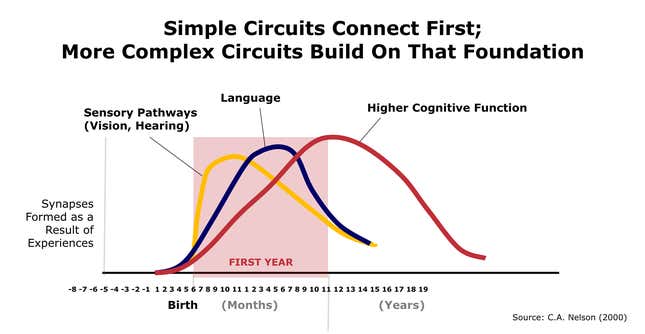
Aceves felt strongly that Juan did not need medicine but more consistent, loving care. Infants need love and tenderness in the same way that they need food. Love and attentive interaction—all that singing and talking and cooing—allows neural networks to build and organize in ways that later make children’s brains more receptive to everything from how to solve a math problem, to how to pay attention in class and manage conflict.
Juan was not getting this kind of care, and Aceves could see that it was having an effect on his behavior. Later, Juan dropped out of school at 14, and at 15, was shot and killed at a party. Aceves remembers getting the call about Juan’s death and feeling a terrible sadness, as well as deep frustration. “We knew that this could happen and we couldn’t change it,” he said.
For years, scientists have been trying to figure out how to break the remarkably robust connection between adversity early in life and bad outcomes later on—poor health, incarceration, dropping out of school, violence. A major pathway through which adversity can cause harm is stress. For some children, the wear and tear of stress on their tiny, fast-changing bodies can become toxic, impairing critical cognitive and emotional foundations. Other children who face similarly hard circumstances will show relative resilience. At present, it is virtually impossible to know which children are most affected by stress and adversity, and thus, which ones are in the most danger.
Aceves is now part of a trail-blazing and controversial group of scientists, pediatricians, and community leaders trying to change this trajectory. They have started to uncover ways to detect which infants are experiencing the effects of stress, and which babies are more resilient. This information could help direct very limited resources to the kids who need it most—if they can find ways to make the measures easy to administer in routine pediatric appointments.
The scientists, a who’s who of leaders in the fields of neuroscience, epigenetics, psychology, and pediatrics, have been working since 2015 to develop a battery of biological and behavioral indicators in children as young as two months and which have now been tested on hundreds of kids in the US. The effort, called the JPB research network, is the first of its kind attempt to identify individual children’s relative vulnerability to hardship so early in life.
The network will test for things like attention and inflammation in infants and young children. We already know that things like how children direct their attention and control their emotions can predict how they do in school, and that persistently elevated inflammation can lead to heart disease, diabetes, and many other chronic illnesses. But by the time doctors and mental-health professionals are able to identify warning signs like inattention and ADHD in kids, it’s through problematic behavior, often around the time children are going to school. To the scientists, this is way too late.
“Self-regulation, attention, and inflammation are to stress as temperature and appetite are to infection,” says Jack Shonkoff, head of the network group, who is also the founder of Harvard’s Center for the Developing Child. In the same way that a fever and loss of appetite are signs and symptoms of illness, a child who shows certain kinds of inattention and inflammation is likely to be experiencing elevated stress. “Without good measurement, we are in the dark.”
To Aceves, the group’s ambitions offer doctors the best chance of moving beyond treating children’s problems as they appear and actually changing the course of kids’ lives. “Maybe with something objective, we can change that reality.”
Looking for the lion
In 1985, Vincent Felitti, a physician and chief of Kaiser Permanente’s Department of Preventive Medicine in San Diego, California, was trying to figure out why more than half the people in his obesity clinic dropped out of the program, even when they were losing weight. Through a fluke—a mis-spoken question—he realized that physical and sexual abuse were far more prevalent than most people thought. He and Robert Anda, an epidemiologist, went on to design a major epidemiological survey at the Center for Disease Control that would play a crucial role in identifying childhood trauma as a root cause for later mental and physical health problems.
Between 1995 and 1997, the study asked 17,421 adults whether they had experienced 10 kinds of trauma as a child, ranging from parents’ divorce to sexual abuse, living with a mother who was a victim of domestic abuse, and emotional and physical neglect. The population of the study was predominantly white (75%) and middle-class. The study then followed the group for 15 years. Nearly two-thirds of Americans had suffered from one “adverse childhood event,” or ACE, and one-fifth had faced three ACEs or more. The more ACEs you had, the more risks you faced down the line. Later studies replicated the findings.
When Anda read the results, he wept. “I saw how much people had suffered.”
Compared with people with zero ACEs, those with an ACE score of four had:
- A 240% greater risk of hepatitis
- Were 390% more likely to have chronic obstructive pulmonary disease (emphysema or chronic bronchitis)
- A 240% higher risk of a sexually-transmitted disease
- Were twice as likely to be smokers
- Were 12 times more likely to have attempted suicide
- Were seven times more likely to be alcoholic
- Were 10 times more likely to have injected street drugs
“I am unabashed about saying it: ACEs are the largest contributor to human disease,” says Pat Levitt, chair of Developmental Neurogenetics at the Institute for the Developing Mind at Children’s Hospital Los Angeles, California, and part of the network.
Soon after the initial ACE findings were published in 1998, neuroscientific research started to unpack the ways in which childhood trauma could land you in the hospital with heart disease at age 50. A lot of roads led back to stress; not everyday stress—the kind that makes you pay attention and work harder—but the kind that sends your body into overdrive, shutting down some systems and hyper-activating others. Over time, with stealth and damning efficiency, this kind of toxic stress can take a toll on the body and mind.
Megan Gunnar, a child psychologist and head of the Institute of Child Development at the University of Minnesota, explains it this way: humans are designed to react to stress. All sorts of circuits and functions in our brains interact to get us to slam on the brakes, or duck, or hide, all in an effort to keep us safe. “We don’t wait until the lion is eating us; at the first sign of the lion, we run the hell away,” she explains.
But when a child lives with abuse, neglect, or is witness to violence, he or she is primed for that fight or flight all the time. The burden of that stress, what Bruce McEwan calls “allostatic load,” can damage small, developing brains and bodies. A brain that thinks it is in constant danger has trouble organizing itself, which can manifest itself later as problems paying attention, or sitting still, or following instructions—all of which are needed for learning. Doing math is difficult when your brain is busy looking for the lion. “What the infant is experiencing in his or her environment, all these traumatic events, is like a rampant infection in a one-month-old; to me that’s physiological trauma,” says Levitt.
The problem is that young children’s stress, much like that of adults, can be invisible. You cannot ask a baby if he is experiencing neglect or abuse; nor do you necessarily know which child is suffering from neglect, abuse, or racism.
“Time does not heal; time conceals,” wrote Felitti, one of the original authors of the ACEs study.
What Shonkoff’s group is trying to do is reveal what can be so damningly concealed.
The key to better treatment
Many kids face adversity and show remarkable resilience, but no one really knows why. Research suggests that the biggest factor in protecting kids from the effects of stress is having a present and loving caregiver, but we can’t yet measure how the presence of a caregiver affects particular biological functions or acts as a buffer against particular kinds of stress.
Unfortunately, ACE tests are not very helpful when it comes to predicting individual susceptibility to problems down the line. First, there’s the problem of disentangling ACE scores. A child who has been sexually abused for years has an ACE score of one; so does a child whose parents have divorced. “It’s never seemed plausible that it’s just the number,” said Charles Nelson, a pediatrics professor at Harvard Medical School, who has, among other things, spent 20 years documenting what happens to infants in severe adversity, including those consistently deprived of attention and care. They also label children and caregivers and and leave out important sources of adversity outside the family, like racism, or community violence.
To scientists, this approach is woefully unscientific. Nelson explains that while there’s a vast and growing literature on the hazards kids face when growing up in poor, low-resource homes, most of that work is behavioral, showing up as impaired executive function or language delays. “That doesn’t tell us why,” he said. It doesn’t explain the biological embedding of stress—how it gets under a child’s skin and affects their behavior—or explain the age at which kids are most susceptible to it.
Michael Meaney, a professor of neurology at McGill University, explains that most common mental health disorders are preventable, if not necessarily curable. But that requires being able to predict who is high-risk. “It’s not that we cannot predict with sufficient accuracy; we cannot predict, period.” He suggests imagining a day-care center with 30 three- and four-year-olds playing joyfully. By the time the same 30 kids hit late adolescence, at least a quarter of them will be suffering from a mental disorder. And yet we don’t know who is at risk.
The matter of measure
Shonkoff’s real innovation may be to try and address all this at once. The point of the group is to have scientists figuring out how to measure stress effects, while pediatricians and community members figure out what treatments are feasible to offer in a visit, and what will be useful to families. “It’s a unique set of relationships Jack has built,” says Levitt. “These groups of people never really come together. Ever. The community is always left out.”
The measures the group is using to test stress are wide ranging. Hair samples allow doctors to test levels of cortisol, which are linked to a person’s ability to learn and adapt to stress. Epigenetic clocks let them see if a child’s body is aging faster than their chronological age would indicate. Inflammatory markers assess stress activation as a physiological response in the immune system; oxidative stress is tested as a measure of cell defense mechanisms. Eye tracking is being used to try and measure attention in babies as young as two months. And EEGs, or brain scans, are looking at the level of electrical activity in the brain to measure the effects of stress, since children who have experienced significant neglect tend to have less electrical activity.
Four years in, the group has made progress. “In the same way we can screen for anemia or elevated lead levels, or the same way we take a temperature if we think someone has infection, we will be able to take measurements of stress effects and resilience in the face of adversity,” says Shonkoff. “That’s never been done before in a validated way in a routine primary care setting.”
But the initiative must consider not just which measures are scientifically accurate, but which ones are realistic to use in a doctor’s office, and that has proven to be tricky. For example, mothers who reported high levels of stress had infants who showed high levels of F-isoprotrane, a measure of oxidative stress. But it was tested through urine, and getting infants to pee on demand proved too tricky, so using the measure as part of a routine primary care visit was tabled. Another issue is cost. Levitt was able to use eye tracking with four-month-olds to detect problems with attention that also correlated to mother’s reported stress. (He found that eye tracking with two-month-olds didn’t work out because their cheeks were too chubby; the infrared beam which measures eye tracking needs a clear path to an eye.) But the tests required computers that cost $12,000, so that had to be set aside until a more affordable system is developed. Cortisol samples from hair were also promising, but many families did not want to give away their baby’s hair.
Some measures look promising. A recent paper published in JAMA Pediatrics shows that the amount of stress that mothers feel was associated with lower brain function in two-month-olds and six-month-olds. “As mom reports more stress and perceives more stress, infants’ brain activity goes down,” Nelson says. That means as early as two months of age, maternal stress is already leading to a reduction in brain activity in the baby.”
It is the first time that such an association has been seen at such a young age. “If you see the effects much earlier like we do, that means you have to intervene much earlier; you can’t wait until they are six or seven,” says Nelson.
But the studies showing that association have been conducted with sample sizes of hundreds. The group now needs to test samples of thousands, then figure out how to move forward on a set of validated measures that can be administered in a pediatrician’s office with families on board.
The goal, Levitt says, is not to come up with 20 stress tests that children have to be subjected to over the course of several years, but rather, “to figure out what we measure at two months that really ends up predictable for issues at two to three years of age.” Once they have that data, they can figure out what to do when the results show elevated stress. “To me the measurements are awesome and important and they will be how we figure out who needs what,” says Kathleen Conroy, a pediatrician and associate clinical director at Boston Children’s Primary Care.
“Now we have to delve into the what.”
The $64-million question
The tests raise some thorny issues. Not everyone thinks more measurement is what children in low-income and deprived areas need. There’s the fear of upsetting or blaming parents, and the possibility that telling parents their kid is stressed out will only stress them out more.
Byron Amos, a community leader in Atlanta, Georgia, who is part of the network, said he is worried about this. “In the real world, if you go to a parent who is doing everything they possibly can to raise their child to say that their effort is hurting their child, you’ve just created more toxic stress.” It’s easy to miscommunicate with parents living in adversity. They haven’t chosen their circumstances, and explaining how those circumstances could potentially harm their babies isn’t necessarily helpful; in fact, it could be quite damaging.
Another concern involves delivering options that aren’t community-led. Frank Oberklaid, director of the Centre for Community Child Health at The Royal Children’s Hospital in Melbourne, argues the push for more screening tools and metrics is misguided. “We’ve been trying to do it this way for 100 years,” he says. “If only we targeted better we’d make a difference; if only we had a better screening test to ID kids earlier, if only we had better interventions. It doesn’t work. There are no silver bullets.”
He is building a model that focuses on working with communities to “co-design” and “co-produce” solutions they want. To give families support, Oberklaid argues “it has to be in the context of a trusted relationship with the family.” Instead of offering prescriptions, people who want to support families ask them what they need, and provide tools that offer it. “The $64 million dollar question is ‘How do we increase the capacity of this family to do better? It’s bloody hard work.”
Shonkoff is aware of these risks and says this is the greatest challenge the group faces: “This must be done in a way that is empowering to parents, and not threatening, especially for parents of color.” It is particularly important, he says, because the US has a consistent history of using poor, marginalized communities of color to advance science often without their permission, or much humanity. “There’s a long history of biology not being used for the good of marginalized groups,” he said.
That presents another challenge: Whether doctors who detect elevated stress have something helpful to offer families. “I don’t think we can offer these measurements without it being paired with something we can do about it,” says Conroy.
After Shonkoff’s group documented the potential harm of toxic stress, it identified three ways to help: reduce sources of adversity; bolster relationships; and improve life skills. Currently, pediatric practices spend a lot of time trying to help families reduce sources of stress—say, helping with housing or making sure there is enough food in the home. There’s less emphasis on working with parents to build life skills like managing their own stress, managing conflicts with their kids, or strengthening family relationships.
And yet research shows that it can be the presence of one loving, consistent adult that can buffer the worst effects of stress and adversity for children. Says Gunnar, from the University of Minnesota: “When the parent is present and relationship is secure, basically the parent eats the stress: the kid cries, the parent comes, and it doesn’t need to kick in the big biological guns because the parent is the protective system.”
But it’s hard to be attentive and responsive to a child’s stress when you are worried about being evicted and where your next meal is coming from. And when the adult is stressed, the baby reacts. “They are not bad parents,” said Gunnar. “They are good parents trying to parent in an awful context.”
To change life outcomes, primary health care may have to expand its role to help build those relationships more.
Conroy is working on how to coach parents on practical, developmental things they can do to help build life skills and strengthen relationships. Reducing adversity is often a systemic rather than individual problem; for many adults, it’s just as important to help them figure out how to parent through it.
In her clinic, many infants appear to be happy, well-adjusted babies who then, at nine months, start showing signs of irregular attachment and dysregulation—that is, not being able to control their emotions in a developmentally appropriate way. Often, Conroy feels the doctors should have been focusing more on attachment and development early on, and parents’ critical role in that.
This means a radical change in primary health care, shifting from health to development, at a time when pediatricians are already being asked to cover a huge swath of issues—health, safety, environmental risks, reading to kids, nutrition, screen time, bike helmets—all in the space of a 10-15 minute appointment.
Conroy says that bringing about such a change means shifting many popular misconceptions: that child development is something that just happens naturally; that babies can’t remember anything, so it doesn’t matter what happens when they are small; that kids really start to learn when they go to school; that success in school is all a matter of tests and grades, which overlooks research that shows that the ability to manage emotions and think flexibly are critically important to kids’ academic outcomes.
An additional challenge is to make sure whatever measures are put in place enhance trust between doctors and families, and not harm them. Power imbalances between doctors and patients–due to race, socioeconomic class, or education–mean that pediatricians need to proceed with caution and consideration for the family’s perspectives. Parents need to be presented with choices, says Nora Razon, manager of community engagement at the Primary School in East Palo Alto. “There are a lot of power dynamics at work and there are a lot of risks,” she said. “It can feel like judgment if there aren’t resources, or next steps; it can harm the relationship.”
Small discoveries and bigger questions
To understand why the world so desperately needs measures of stress in infants and young children, Shonkoff likes to tell the story of acute lymphoblastic leukemia (ALL), the most common cause of cancer in children.
Fifty years ago, the survival rate for ALL was 3%. By 1975, it was 60%. Today, it is over 90%. Over the past 30 years, there has not been a single new treatment for ALL, but rather a revolution in how we understand different subtypes and how they respond to different treatment options. Indeed, it is not one disease, for there are variants. By understanding the variants, the biology of the cancer cell, and individual variation in children’s responses to different treatments, doctors can target the disease effectively. “This is the heart of precision medicine,” says Shonkoff: Segmenting the disease; segmenting risk; analyzing differential response.
“The field would like to get where cancer is,” says Nelson. “Depending on what genotype you have, you get a different treatment.” Instead of saying that a child has a high ACE score because he lives in a violent neighborhood and has been emotionally neglected, the goal is to identify exactly what impact adversity is having on him and find a way to treat it. You identify the brain circuit that is impaired—say, language development—and target that, rather than saying, “Your child is stressed out, try language therapy.”
One critical question is what other factors beyond stress are at play in shaping children’s development. “If you just reduce the stress in the household—but they are still poor and uneducated—would the kids develop perfectly fine? I am skeptical, I don’t think it’s that simple,” says Nelson.
At the end of the day, the group is trying to do way more than measure stress. It is trying to answer some of society’s hardest questions right now: Why do so many poor children get sick compared to wealthy kids? Why do they struggle in school? Racism and social class play a role, but what role—and how do you work to change the reality that a mother’s education and zip code so profoundly influence her children’s health? In the US, while poverty rates have improved over the past few decades, the pattern by which family income dictates children’s outcomes—from graduation rates to employment, health, and happiness—has actually gotten worse.
Amos, the community leader in the network in Atlanta, Georgia, says when he was first approached to be part of the group, he was skeptical about the utility of the project: “Let’s spend the money on getting rid of toxic stress and not worry about the biological markers.” Wouldn’t it be better to devote resources instead to things like access to affordable housing, improving public schools, and getting grocery stores with fresh produce into low-income communities?
But as he spent time with the group, he decided that combining forces with people from so many different fields, from scientists and doctors to folks like him, might be a smart way to address the complex web that is poverty. Changing society and structural poverty and racism will take generations. While it’s a worthy endeavor, people who are alive today also need ways to cope with the adversity they’re living with.
He says his involvement with the group has already given him additional tools to advocate for his community with cutting-edge science. For example, he’s fought for more recess in public schools for years: Now the demands are more scientific. “This [network] is one of the first times I have seen this holistic approach,” he says.
The group has moved from its first three-year phase of developing preliminary measures with pediatricians and community leaders to continuing that work while also creating an effort called the Pediatric Innovation Initiative, which will look at the bigger practical question of how to employ new measures effectively in a diverse set of communities. They are seeking more pediatric practices to partner with to give feedback on what’s feasible and involve a broader range of families in the studies. The group met last week and agreed to keep testing the measures to see what might work in a doctor’s office, as well as start working on the language that will be needed to communicate to parents complicated, and sometimes, scary information.
Like all good science, small discoveries lead to bigger questions. Where is the best place to support families? In the home or in the doctor’s office? At what age, and for what issue? “We don’t know any of these,” says Nelson, who is optimistic about the project, but cautious as scientists are prone to be.
There is no immunization or treatment that a doctor can offer against getting shot at age 16. But certainly more could have been done between that first visit to the pediatrician when Juan was born, and the day he died. Figuring out exactly how to provide parents and kids with the help they need is, as Oberklaid says, bloody hard work.
Read more from our series on Rewiring Childhood. This reporting is part of a series supported by a grant from the Bernard van Leer Foundation. The author’s views are not necessarily those of the Bernard van Leer Foundation.